The Challenge: Measuring Success in High-Risk, Community-Based Care
Psychiatric Rehabilitation Programs (PRPs) serve individuals with serious and persistent mental illness who often require long-term, community-based support. Unlike traditional outpatient therapy where success is focused on measurable symptom improvement, success in PRP settings is defined by stability, functional improvement, and prevention of crisis escalation.

Partnership Development Group, Inc (PDG) provides psychiatric rehabilitation, case management, and related mental health supports across Maryland. Their staff (largely bachelor-level direct care providers) work independently in the field, often meeting with clients multiple times per month to support normal daily activities, medication adherence, benefits navigation, and coordination with community providers.
Working with this population and delivering care through this model presents several challenges:
- Limited real-time visibility into client risk, including psychiatric escalation between visits.
- High variability in documentation results in inconsistent visibility into client status, especially across a distributed, field-based workforce.
- Difficulty reporting objective outcomes when success is focused on preventing crises.
- Persistent risk of high-cost emergency department (ED) visits and inpatient admissions, resulting in care disruption, instability, and increased system burden.
Like many PRP providers, PDG needed a way to identify risk earlier, consistently monitor client symptoms throughout care, and demonstrate the value of their services, without adding clinical burden or forcing a traditional therapy model onto PRP care.
The Approach: Embedding Measurement-Based Care Into a Non-Traditional Clinical Model
In September 2023, PDG implemented Greenspace’s Measurement-Based Care platform across its PRP services to bring structure, consistency, and visibility into client progress and risk. Rather than forcing a traditional therapy model onto PRP care, PDG tailored MBC to fit their setting by:
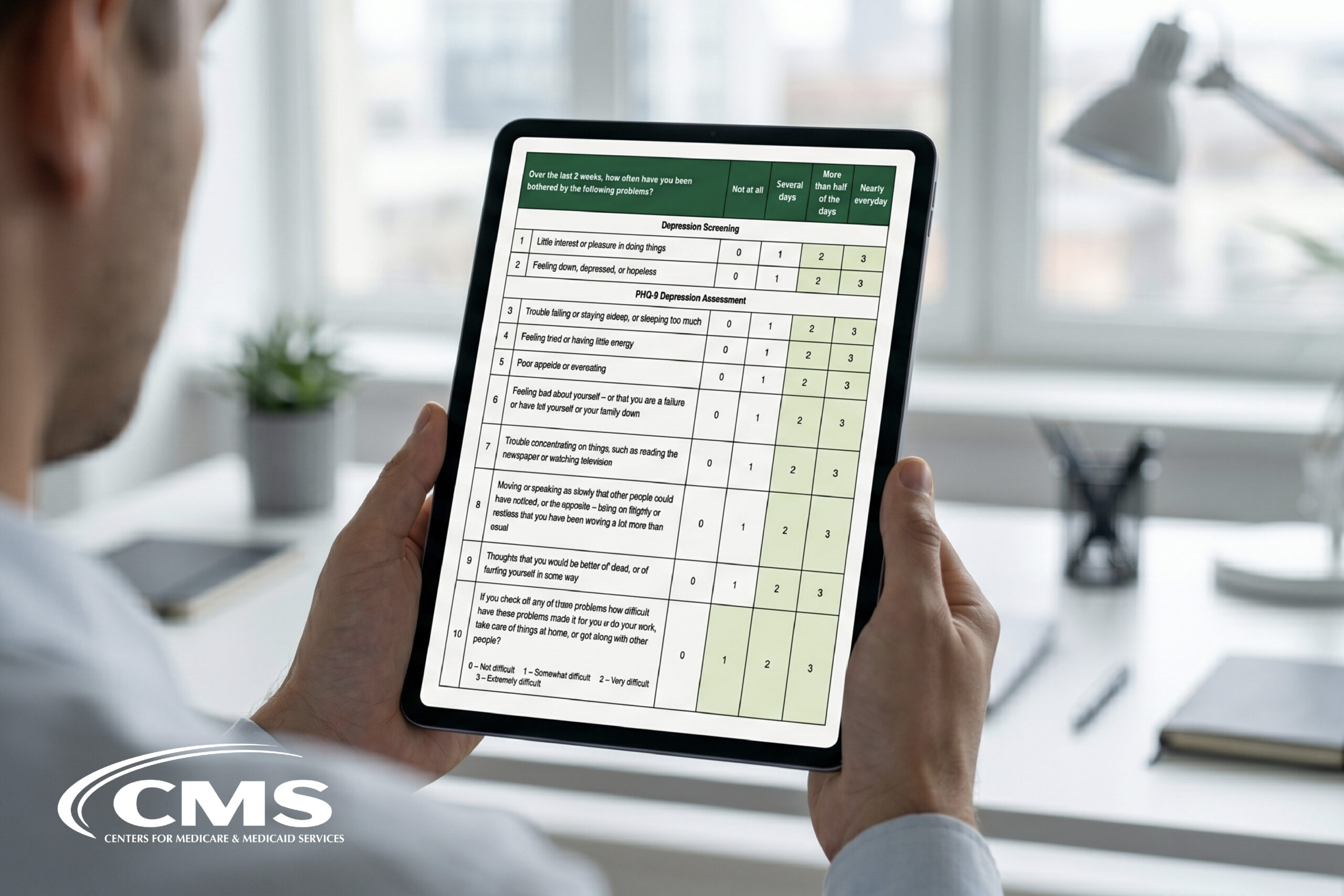
- Using brief, validated assessments appropriate for community-based care, including the PHQ-9, GAD-7, WSAS, and the BR-WAI.
- Empowering direct care staff to collect outcome data during routine field visits to support care conversations.
- Using Greenspace to standardize monitoring across clients, regardless of role or location.
- Enabling providers and supervisors to use real-time data to inform care decisions, identify emerging risk, and intervene earlier.
PDG’s implementation goal was not to reduce acuity overnight. Instead, they wanted to drive greater client stability and ensure clinical outcomes were measurable and reportable. Their implementation focused on improving visibility, consistency, and clinical decision-making in a high-risk population, with stability as the primary indicator of success.
Adoption & Engagement: Consistent Measurement at Scale
Since launch, PDG has demonstrated strong and sustained engagement with MBC:

This level of engagement reflects PDG’s ability to operationalize MBC within a community-based model, ensuring that it helped strengthen clinical decision-making by providing objective structure and visibility into client progress.
The Impact
From Visibility to Early Intervention
For PDG, Greenspace enabled:
- Earlier identification of risk across a distributed workforce
- Consistent monitoring without increasing the documentation burden
- Stronger supervision and care coordination
- A defensible way to demonstrate value in a setting where stability, not discharge, is success
Rather than replacing clinical judgment, MBC helped to strengthen clinical judgement by providing the structure and objective insights to inform clinical discussions and decisions in a setting where traditional models have fallen short.
ROI Through Prevention
Psychiatric emergency department visits and inpatient admissions are among the most resource-intensive events in mental health. A reduction in utilization in a population with elevated baseline risk reflects a meaningful decrease in high-cost acute care, even when overall acuity remains stable.
In high-risk community-based care, a key part of ROI is continuity of treatment. At PDG, more than 36% of clients completed ten or more assessments throughout care, surpassing the broader Greenspace average of 29%. In a PRP setting, that level of sustained measurement supports strong longitudinal visibility into client needs and helps to ensure early intervention before risk escalates into costly acute care and treatment interruptions.

Zooming out across all PRP programs that Greenspace provides MBC infrastructure for, outcome trends reflect this reality. After five sessions of care, 95% of clients maintain stability or reliably improve on the PHQ-9 and 93% on the GAD-7. In a population where maintaining community stability is often the primary goal of care, this represents a meaningful indicator of high-quality, effective care.
Controlled Psychiatric Emergency Utilization in a High-Risk Population
To better understand system-level impact of MBC, PDG analyzed internal incident reports alongside state-level utilization data, examining psychiatric emergency department visits and inpatient admissions before and after their implementation.
Following implementation in 2023, PDG observed a continued decline in psychiatric emergency department and inpatient incidents, from approximately 2.3% in 2023 to 1.5% in 2024. This represents a ~35% relative reduction in psychiatric ED and inpatient admissions year over year. Reports of suicidal ideation increased following implementation, reflecting improved identification and monitoring of risk through ongoing outcome measurement rather than an increase in crisis frequency.
Importantly, this trend occurred in a population with structurally elevated risk, where escalation is common and often difficult to prevent.
System-Level Financial Impact
Published benchmarks suggest:
- Psychiatric ED visits often cost hundreds of dollars per visit (commonly ~$520–$600+, depending on payer and setting).
- Inpatient stays for mental or substance-use diagnoses can average several thousand dollars per stay.
If a mental health organization serving 10,000 clients experienced a 35% relative reduction in psychiatric ED and inpatient events over the course of a year (for example, declining from 3.0% to ~2.0% of clients experiencing an event) that would equate to approximately 100–110 fewer high-acuity events annually.
Using conservative per-event cost proxies (e.g., $600–$700 per psychiatric ED visit and $8,000–$10,000 per inpatient admission), even modest reductions in utilization of this magnitude could represent meaningful reductions in cost exposure, particularly when inpatient admissions are avoided.
At $600 per ED visit, this would represent approximately $60,000 annually in avoided ED visit costs alone, with materially higher impact if inpatient admissions are reduced.
Realize the full financial impact of Measurement-Based Care.
Drag the slider for a snapshot. For a detailed, custom breakdown, try the full ROI calculator.
Looking Ahead: A Model for PRP and Community-Based Care
PDG’s experience demonstrates how MBC can be successfully adapted to non-traditional mental health settings, supporting stability, accountability, and cost containment without disrupting care delivery. As states and funders increasingly focus on outcomes, risk management, and efficient use of resources, MBC offers PRP providers a practical, scalable way to show the impact of their service across both client outcomes and reduced healthcare costs.
Try our ROI Calculator to explore the potential ROI of MBC at your organization, or schedule a call with an implementation expert.