The correlation between depression and diabetes.
Mental illness and chronic physical illness are not only co-existent, but are in many cases co-dependent. On the one hand, mental illness makes patients susceptible to poor physical health, a core component of managing chronic illness. As an example, obesity rates are up to 3.5 times higher among people living with serious mental health illness according to the Canadian Journal of Psychiatry. 1
In looking at the reverse correlation, many studies have evidenced that chronic physical illness creates a significantly higher probability of developing mental illness. Statistics Canada published a health report stating that “women with depression are 80 percent more likely to have heart disease than women without depression.” 2
A close link between mental and physical illness is also seen in the case of diabetes and depression. Studies have concluded that patients diagnosed with type 1 diabetes are up to 3 times more likely to experience depression , and are therefore at a higher risk of poor self-care and treatment nonadherence. 3,4
How medication affects this relationship.
Regular medical regimen is necessary to maintain balanced blood sugar levels for diabetic patients, and thus treatment adherence is integral to proper management of diabetes. Diabetic patients suffering with depression have a higher likelihood of missing doses or taking them at delayed times, causing disturbances in their treatment plans.5 This presents a challenge to the patient’s ultimate wellbeing and can also have further adverse effects on his or her physical and mental health.
In addition, negative side-effects of psychiatric medications can include an impact on weight gain.1 This means that antidepressants may worsen a diabetic patient’s physical condition and therefore interfere with other treatment goals.5
What does this mean for treating diabetes?
Primary care providers are typically the first to diagnose chronic physical illness and this puts them in a position to identify associated indications of mental illness at an early stage. However, this comes with its challenges. A publication in the Canadian Journal of Psychiatry illustrated how diagnostic overshadowing (when identifying a physical illness) could mask psychiatric complaints, especially in mild and moderate mental illnesses.5
Further, depression has a meaningful impact on treatment adherence. If a patient’s mental illness is not understood in the context of chronic physical illness, the management of disease is less likely to be successful. In the case of diabetes, treatment failure may be attributed to conditions of depression that hinder an individual’s motivation for self-care. This self-care includes exercise, a balanced diet, and compliance with medications; all key components of treating diabetes.4 As an example, diabetic patients with major depression were nonadherent to oral medication on 24.5 percent of days.6

As a result, a holistic approach that includes the early detection of mental illness is critical to promoting the overall wellbeing of a patient. As healthcare providers become aware of this important correlation, they might choose to consider some of the following options for patients:
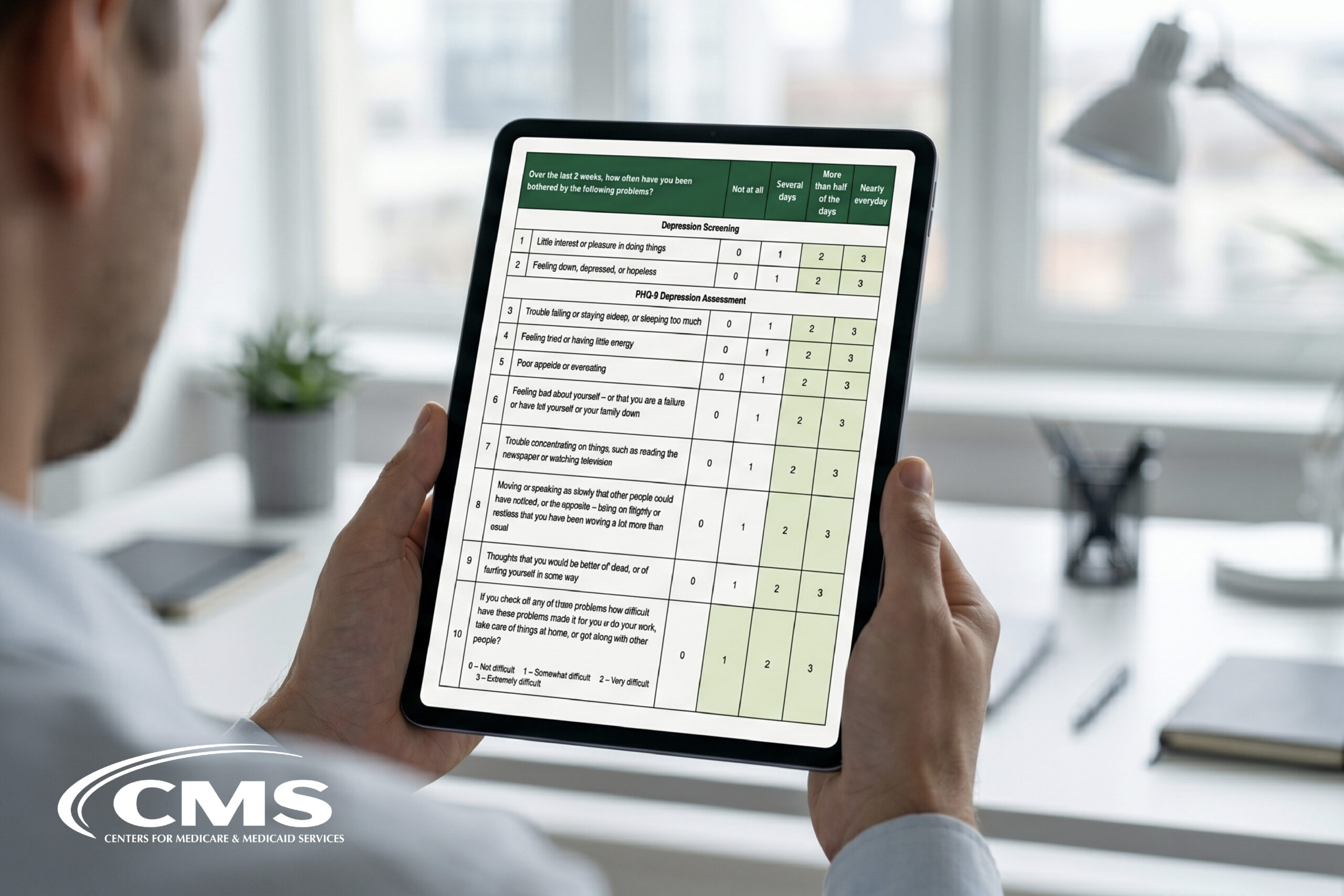
- Screen: Conducting a regular screen for depression and anxiety with tools like the PHQ-9 and GAD-7 will help to overcome the challenge of diagnostic overshadowing.
- Therapy: Recommending a course of evidence-based psychotherapy in order to treat depression symptoms. In some settings, there are group programs specific to diabetes self-management that include a mental health component.
- Medication: When choosing to prescribe medication for depression, it is important to consider whether weight-gain is a negative side-effect.
- Collaborative Care: Working with other healthcare providers and improving the sharing of mental health information has been demonstrated to benefit patient care.
Given what we know about the correlation between chronic physical illness and mental illness, it is no longer possible to treat diabetes without a focus on patient mental health. While community-based programs and ministry initiatives will evolve to better support patient needs, it is important for primary care providers to initiate this conversation today.
—
References
1 S. Coodin, “Body Mass Index in Persons with Schizophrenia,” Canadian Journal of Psychiatry 46 no. 6 (2001): 549‐555.
2 H. Gilmour, “Depression and Risk of Heart Disease,” Health Reports, 19, no. 3 (July 2008), Statistics Canada, Catalogue no. 82‐003‐XPE
3 Roy T, Lloyd CE. Epidemiology of depression and diabetes: a systematic review. J Affect Disord. 2012;142(Suppl):S8–S21
4 Gonzalez, J. S., M. Peyrot, L. A. Mccarl, E. M. Collins, L. Serpa, M. J. Mimiaga, and S. A. Safren. “Depression and Diabetes Treatment Nonadherence: A Meta-Analysis.” Diabetes Care 31, no. 12 (2008): 2398-403. doi:10.2337/dc08-1341.
5 Canadian Mental Health Association Ontario. “The Relationship between Mental Health, Mental Illness and Chronic Physical Conditions.” December 2008, 1-9.
6 Lin, E. H.b., W. Katon, M. Von Korff, C. Rutter, G. E. Simon, M. Oliver, P. Ciechanowski, E. J. Ludman, T. Bush, and B. Young. “Relationship of Depression and Diabetes Self-Care, Medication Adherence, and Preventive Care.” American Diabetes Association Diabetes Care 27, no. 9 (2004): 2154-160. doi:10.2337/diacare.27.9.2154.