Over the last decade, Ohio has experienced a growing mental health crisis coupled with a major opioid epidemic. It has become clear that the system of care across the state is in need of a comprehensive plan to strengthen its mental health infrastructure, improve access, and ensure everyone in Ohio is receiving the level of care they need to thrive. In response, the Ohio Council of Behavioral Health & Family Service providers released a number of policy solutions to lay the groundwork for a more effective health system.
Our partners at the Ohio Council proposed 8 major solutions to help tackle the mental health crisis. These solutions address a wide-range of factors, from adjustments to better support the behavioral health workforce and improve treatment access, to statewide prevention efforts and infrastructure innovation.
With any report of this scope and complexity, it can be difficult to picture what these recommendations can look like in practice. There are some standout themes, topics and ideas throughout the report that we find particularly interesting and have pulled out and highlighted below, along with our thoughts of how they can actually be applied in practice.
If you’re interested in reading the full report, you can find it here.
1. School-Based Interventions, Meet MBC
The impact of the pandemic on school-aged children’s mental health is becoming more apparent, and the demand for school-based interventions is rising. According to a 2020 analysis from the CDC, of the school-aged children in Ohio who needed mental health treatment only about 1 in 5 received professional support, and this is prior to the steep rise in service demand during and post-pandemic. Now that many young people are returning to in-person classes and the impact of the pandemic on their mental health is becoming more apparent, it is fitting that the Ohio Council’s efforts towards statewide prevention are largely school-based.
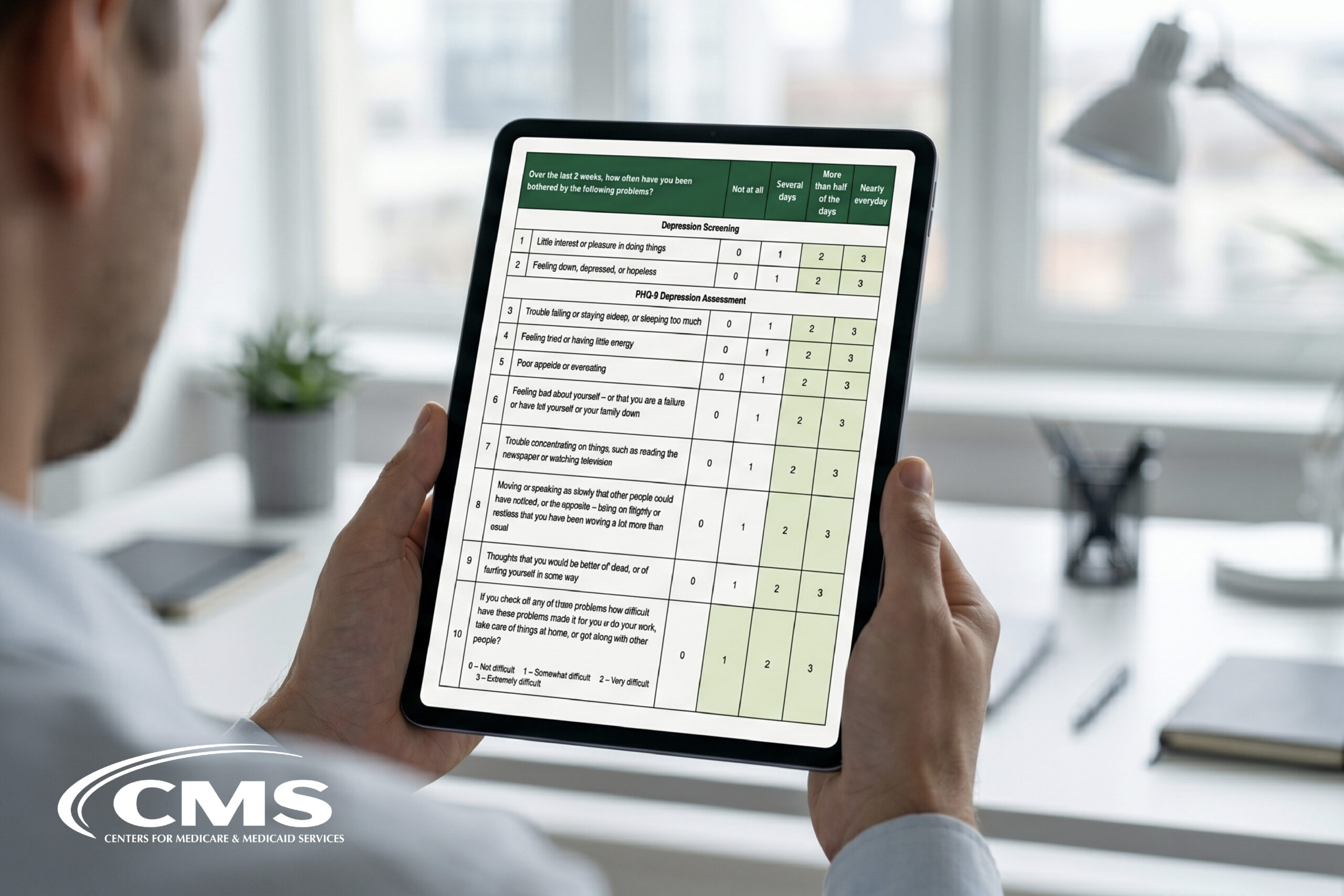
The Ohio Council’s recommendations promote improved access, a more comprehensive range of services, large-scale awareness efforts, and school-based mental health screening. Implementing any one of these solutions is a step in the right direction, especially if Measurement-Based Care (MBC) is built in from the start to ensure we understand which services are preferred by young people, which are most effective and why. With MBC, decision makers will be able to understand how the interventions they’ve invested in are improving the lives and the well-being of their population, and make adjustments, innovations, and iterations to available services based on needs identified directly by the young people they’re working to support.
In addition to prioritizing improved student mental health services, it’s great to see a focus on awareness. We’ve seen in our school-and university-based implementations that a few vital keys to prevention are ensuring that:
- Students know exactly where to go to access the virtual or in-person mental health support available to them, making appropriate services easy to navigate and;
- Students are given an opportunity to engage with their mental health proactively, before they’re in need of support. This includes tools to help them reflect on their mental health, and better understand what influences their ups and downs over time;
- Teachers, professors and staff feel comfortable directing students to one central place where they are confident students will find the support they need, regardless of where they currently are in their mental health journey.
2. High Waitlists = Low Access; Insert CCBHC’s
One of the biggest issues facing Ohioans is the lack of access to care, generally. The Ohio Council shared some statistics that paint a striking image of the level of need in the state:
- Prior to Covid-19, only 40% of those with mental health conditions obtained care;
- Prior to Covid-19, only 10% of those with a substance use disorder found their way to treatment;
- In 2020, only 20.3% of adults with a mental illness had received any mental health treatment in the past 12 months.
One of the major contributors to this low access to care is long wait times to get treatment. In fact, the average wait time for treatment across the US is 48 days. Seeing as this is a national problem, many states have been working to find solutions. Some have seen massive waitlist improvements after launching Certified Community Behavioral Health Centers (CCBHCs), reducing wait time to care to 10 days or less, which is exceptional in comparison.
CCBHCs combine a variety of treatment specialists into one 24-hour location, allowing people to be treated for both mental and physical health concerns, all in one visit. This type of model is extremely valuable when we consider that mental health, nutrition, addiction and physical health all generally effect one another and can compound and increase the impact and amplitude of one another.
3. Integrated Care
Another major barrier to broad access highlighted in the report is the lack of a full continuum of accessible and connected behavioral and physical health services. Various communities in the state, particularly rural areas, don’t have access to effective prevention, crisis response, treatment, and/or recovery support services.
The Ohio Council’s recommendation is OhioMHAS certification and Medicaid coverage of CCBHCs or similar integrated and collaborative, whole-person care delivery models, particularly for people with chronic mental illness and substance use disorders. The reimbursement model—which divides total operating costs by number of visits, using the rate per visit— is more flexible than the regular fee-for-service model. This way, facilities can adapt their services to the unique needs of individual communities, based on the actual costs associated with running a facility in that area (facilities in a centralized city typically have higher overhead and experience more visits then ones in small counties, for example).
While this may increase initial costs for service delivery, down the line there would be significant cost savings. This is due to the reduction of hospitalizations and emergency room visits for mental health services, but also in the reduction of physical health care costs that are exacerbated due to mental health struggles which, in an integrated model, can be discovered and treated earlier.
Developing an effective and accessible integrated care model is fundamental to ensuring that health care is person-centered and is effective across an entire population. By coordinating behavioral and physical health, you can better treat the whole person— especially the many individuals who experience concurrent mental and physical health issues.
4. Data
While all of the above solutions will benefit from a comprehensive set of evaluation data and insights, a key recommendation from the Ohio Council sets expectations for what this should look like across the state. The recommendation is to develop a uniform, consistent, and statewide set of data and metrics to be collected and shared with appropriate interested parties.
The collection of consistent patient-reported data through a process like Measurement-Based Care (MBC) helps to improve treatment outcomes and drives a higher standard of care across the state. MBC has been shown to reduce dropout and cancellations by 40% (Bohanske & Franczak, 2010) and increase symptom improvement by 42% (Lambert, 2013). Effective implementation of MBC would also increase the states ability to understand the effectiveness of services, iterate to ensure they’re providing the best care possible to the population they serve and better understand which services should be prioritized under a Value-based Care model. A collaborative approach to patient-reported data collection is an exceptional opportunity for providers across the state to collect clinically-useful data, create benchmarks, and share learnings to drive improved service effectiveness and resource allocation across Ohio.
5. Set Standards
In order to ensure a high standard of care across any state or region, there should be established requirements that all organizations must meet. To promote quality and adherence, the Ohio Council has recommended instituting recognized standards of care and service delivery through behavioral health national accreditation.
As long as the standards outlined by the accrediting body are a) relevant and helpful to the service providers delivering care and b) the reporting requirements chosen actually reflect the goals of different types of treatment, this can be a vital step in improving the quality of care in a consistent way across Ohio.
More accrediting bodies, like the Joint Commission, have been adding Measurement-Based Care as a requirement to evidence-based practice. This is a good example of a standard that is useful in both reporting and in practice. By design, MBC measures what matters, as it uses patient reported outcome measures (PROMs) that are responsive and flexible based on an individual patient’s presenting symptoms and personal goals. This not only helps inform treatment, but it’s also beneficial when trying to understand if treatment is effective and why it may, or may not, be working for a particular individual, specific type of issue or across an entire population.
Final thoughts
Though Ohio’s behavioral health and substance use crisis has gotten worse over the years, this can be seen across North America as well. The Ohio Council’s report is evidence that work is being done to address and overcome these challenges together. This collaborative approach is going to be fundamental to improving mental health service delivery generally, but also in better supporting the overall mental and physical health of people across Ohio. We’re proud to be partnered with the Ohio Council and to support organizations in the state who are working to implement MBC to increase the quality of care they deliver.
To learn more about Measurement-Based Care, visit our ‘What is MBC?’ page or reach out to info@greenspacehealth.com talk to an MBC implementation expert today.
References
Ohio Council of Behavioral Health & Family Service. (2022). Policy Solutions for Ohio’s Mental Health & Substance Use Disorder Crisis. https://www.theohiocouncil.org/assets/WhitePaper/Whitepaper-Policy-Solutions-for-Ohios-MH-SUD-Crisis-August-2022.pdf
Bohanske, R. T., & Franczak, M. (2010). Transforming public behavioral health care: A case example of consumer-directed services, recovery, and the common factors. In B. L. Duncan, S. D. Miller, B. E. Wampold, & M. A. Hubble (Eds.), The heart and soul of change: Delivering what works in therapy (pp. 299–322). American Psychological Association. https://doi.org/10.1037/12075-010
Lambert, M. J. (2013). Outcome in Psychotherapy: The past and important advances. Psychotherapy, 50(1), 42–51. https://doi.org/10.1037/a0030682