Q&A from 'Advancing Substance Use Disorder Treatment Through Measurement-Based Care'
In our recent educational webinar, Advancing Substance Use Disorder Treatment Through Measurement-Based Care, we were joined by three leading experts in behavioral health and implementation science: Dr. Kelli Scott, Assistant Professor at the Center for Dissemination and Implementation Science at Northwestern University Feinberg School of Medicine and Principal Investigator at the Healing Measurement Center; Dr. Sandra Resnick, Professor of Psychiatry at Yale University and co-founder of the Yale Measurement-Based Care Collaborative (Yale MBCC); and Dr. Jessica Barber, Clinical Health Psychologist and co-founder of the Yale MBCC.
Together, they explored how MBC can be thoughtfully applied in SUD treatment settings, what makes implementation distinct in this context, and how organizations can take measurement beyond reporting to becoming a genuine clinical tool.
The session generated an enormous volume of questions from attendees across North America. We didn’t have time to address all of them live, so we’ve pulled together responses below, organized by theme. We hope this serves as a practical resource for anyone implementing or expanding MBC within substance use disorder services.
Need a refresher? You can access the full recording here.
Why MBC in SUD? The Core Case
What makes MBC uniquely valuable in SUD treatment, compared to general behavioral health settings?
Recovery from substance use disorders is often non-linear, and progress doesn’t always look like abstinence or reduced use alone. MBC gives clinicians and clients a way to track multiple dimensions of that journey, including quality of life, functioning, social connection, and values-based indicators of recovery, rather than focusing narrowly on substance use metrics.
As Dr. Barber noted during the webinar, measures of quality of life and recovery can surface deeply personal information: what matters most to a client, where they find happiness, what they’re working toward. This aligns naturally with motivational interviewing and strengths-based approaches that are central to effective SUD care. It also allows clinicians to balance difficult, sometimes stigmatizing conversations about substance use with more empowering and holistic check-ins.
Dr. Scott added that MBC is particularly useful for assessing risk, including potential for return to use and overdose, in a setting where the overdose crisis continues to affect communities across North America. MBC creates a structure to monitor both progress toward recovery and emerging warning signs, supporting a harm reduction orientation alongside clinical decision-making.
How does MBC support clinicians who are managing large caseloads with limited time?
This came up repeatedly in the session, and it’s one of the most practical arguments for MBC in SUD settings. Dr. Scott described working in opioid treatment programs where counselors may carry caseloads of 70 or more clients and meet with individuals for as little as 30 minutes per month. In that context, MBC helps clinicians quickly orient to how a client is doing, identify the most pressing topic for today’s session, and flag clients who may need more intensive support, all without relying on memory alone across a large and complex caseload.
Far from adding burden, a well-implemented MBC process becomes a clinical efficiency tool. As Dr. Scott put it, MBC can actually save time in the end because it helps clinicians check in quickly and direct their attention to what matters most.
Selecting the Right Measures
Given the wide range of validated SUD screeners available, what instruments would you recommend for tracking treatment response and recovery over time?
This was the most upvoted question in the session, and the panelists were deliberate in their response: there is no single gold-standard measure for MBC in SUD care, and focusing too much on finding the “perfect” measure can be a barrier to getting started.
Dr. Resnick put it plainly: the magic is not in the measure, it’s in the conversation. That said, she acknowledged that the closer a measure is to what you’re treating and what your clients care about, the richer the discussion it will generate. Any measure that is broadly in the right domain will provide value when you commit to the full Collect, Share, Act process; collecting the data, sharing it back with clients, and actually doing something with it.
Dr. Barber recommended evaluating measures by imagining the conversations they could open up. Look at the individual items on a measure, not just the total score. Ask yourself: could these questions lead somewhere productive? Do they cover things I know matter to my clients but that don’t always come up naturally in session? Are there domains (like happiness, quality of life, or social functioning) that would add a strengths-based dimension to otherwise symptom-focused conversations?
For quality of life and recovery, the panelists referenced measures that assess domains such as doing things that are important to the person, positive experiences, and overall wellbeing. The Quality of Life in Recovery (ReQoL) measure is one example Dr. Barber uses regularly in her own clinical practice.
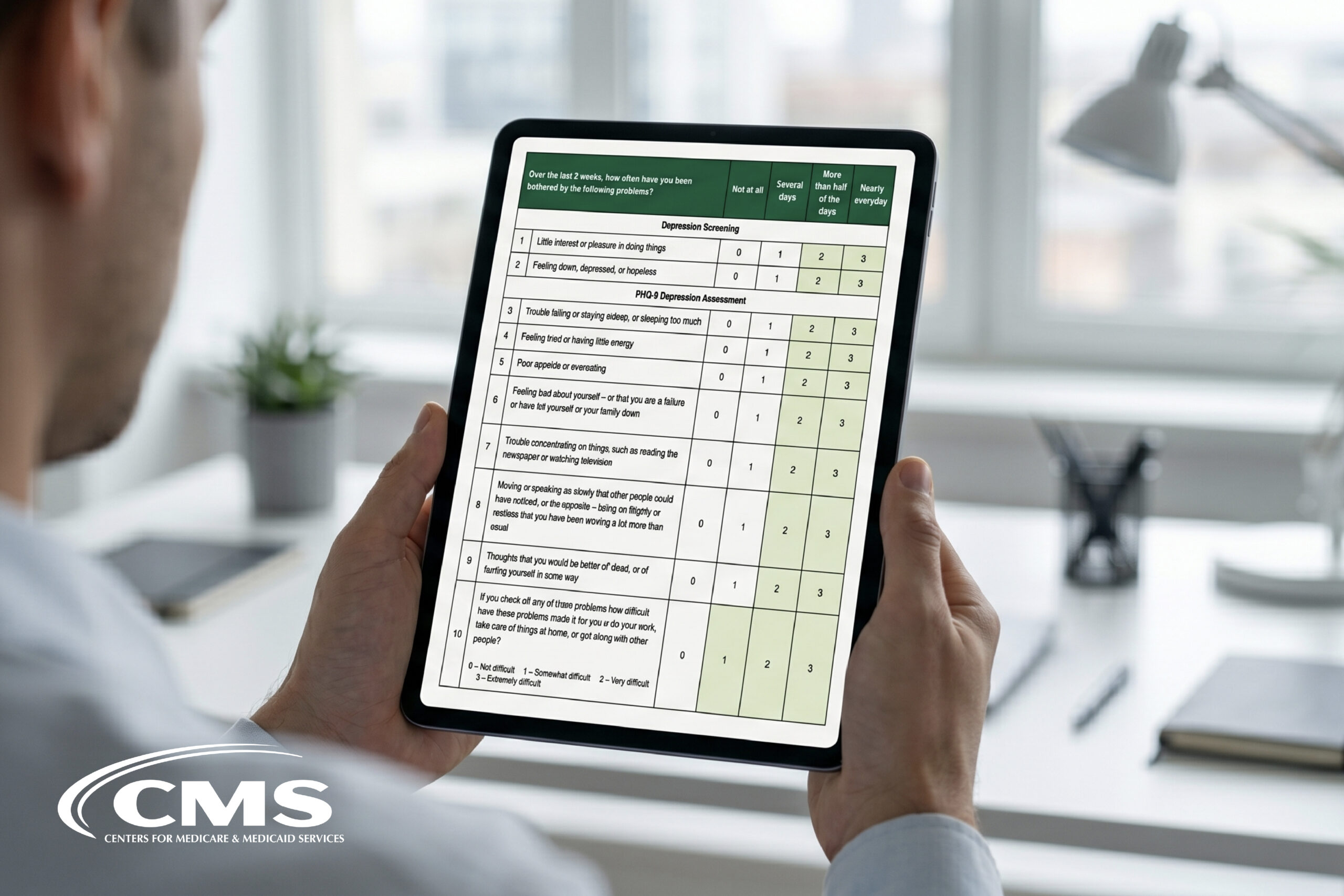
For symptom monitoring, tools like the PHQ-9 (depression) and GAD-7 (anxiety) are widely used and well-validated across behavioral health and SUD settings. The Brief Addiction Monitor (BAM) and AUDIT-C are among the tools designed specifically for SUD contexts and are commonly used to monitor substance use and related functioning.
For recovery capital, a dimension several attendees specifically asked about, measures like the Assessment of Recovery Capital (ARC) and the Brief Assessment of Recovery Capital (BARC-10) are designed to assess internal and external strengths that support recovery. These are well-suited to a holistic, strengths-oriented approach to SUD care.
What patient self-report measures would you recommend for SUD, specifically those that are validated and don’t require clinician administration?
Several participants noted they find it difficult to identify self-report SUD measures that are both psychometrically sound and practical for routine clinical use. A few options worth considering:
- The AUDIT (Alcohol Use Disorders Identification Test) and DAST-10 (Drug Abuse Screening Test) are brief, validated, and widely used self-report tools for identifying problematic alcohol and drug use, respectively.
- The BAM (Brief Addiction Monitor) is a 17-item self-report tool developed by the VA that covers substance use, risk factors, and protective factors relevant to recovery — making it useful for ongoing monitoring, not just screening.
- The PROMIS Substance Use item banks offer flexible, validated self-report options developed through NIH-funded research, including computer-adaptive testing versions that reduce respondent burden.
- For recovery-oriented monitoring, the BARC-10 mentioned above is also self-report and brief enough for routine use.
The key principle from the panelists: choose a measure you can commit to using consistently, that generates conversations your clients find relevant, and that fits within your workflow. Psychometric quality matters, but uptake and clinical integration matter just as much.
What quality of life measures are under 12 items and in the public domain?
A few strong options:
- The EQ-5D-3L is a five-item, public-domain quality of life measure widely used in health research and clinical settings. It covers mobility, self-care, usual activities, pain/discomfort, and anxiety/depression, with a visual analogue scale for overall health.
- The WHODAS 2.0 (12-item version) assesses functioning and disability across six domains. It is free to use and available from the World Health Organization.
- The Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS) is a 14-item (or 7-item short form) measure of positive mental wellbeing. The short form is available for free in most clinical and research contexts.
For SUD-specific contexts, the Quality of Life in Recovery (QLIR) referenced earlier is another option, though item count varies by version. The Yale MBCC and Greenspace’s Assessments Hub can provide further guidance on measure selection, including licensing and administration details.
How do you view recovery capital tools like the ARC and BARC-10?
Recovery capital measures are a natural complement to MBC in SUD settings. Rather than focusing solely on symptom reduction or abstinence, recovery capital tools assess the internal and external resources a person draws on to sustain recovery, including things like social support, housing stability, engagement with community, and self-efficacy.
This aligns directly with what the panelists emphasized throughout the webinar: MBC in SUD care is most valuable when it captures the whole person, not just the substance use. Recovery capital measures can surface client strengths, track positive momentum even when other indicators are mixed, and support values-based conversations that build motivation and therapeutic alliance.
The BARC-10, in particular, is brief enough for routine use and has demonstrated good psychometric properties in research settings. The ARC provides more granular detail across multiple domains and may be better suited to initial assessment or periodic in-depth check-ins, rather than every-session monitoring.
What screening tools do you recommend for adolescents and teens?
For adolescents, a few tools are well-supported in research:
- The CRAFFT (Car, Relax, Alone, Forget, Friends, Trouble) is one of the most widely used and validated screening tools for substance use among adolescents aged 12–21. It is brief (six items), free to use, and available in multiple languages.
- The POSIT (Problem Oriented Screening Instrument for Teenagers) provides a broader assessment across functional domains, including substance use, mental health, physical health, family and peer relationships, and vocational status.
- The PHQ-A (Adolescent version of the PHQ-9) and GAD-7 are appropriate for co-occurring depression and anxiety monitoring in teens.
For programs working with youth, Dr. Scott and the Yale MBCC team emphasize that the same principles apply as with adults; choose measures that generate clinically useful conversations, involve young people in understanding and interpreting their scores, and remain flexible to the developmental context.
Does research support the use of MBC with youth who misuse substances?
The research base for MBC in adolescent SUD treatment is more limited than in adult populations, but growing. Studies of routine outcome monitoring and feedback-informed treatment in youth behavioral health broadly, including substance use, have shown promising results for improving engagement, identifying non-response early, and supporting treatment planning. The mechanisms are largely consistent with the adult literature: regular check-ins improve alliance, make progress visible, and support timely adjustments when treatment isn’t working.
Involving caregivers is an important dimension for adolescent SUD care. While this does add some complexity, particularly around confidentiality, it can also strengthen outcomes by ensuring families are informed and engaged. See the question below on caregiver inclusion for more on that.
Measurement-Based Care with Greenspace
Ready to see what Measurement-Based Care could look like at your organization?
Schedule a CallImplementation: Making It Work in Practice
In a specialized MHSU tertiary care setting, how do we refine the choice of instruments? Should there be program-level measures or more individualized measures? And how much measuring is too much?
This is one of the most thoughtful implementation questions that came up, and the panelists addressed it directly during the session.
Dr. Resnick shared that even when organizations have large libraries of available measures, clinicians tend to gravitate toward a small handful of them. You don’t need an overwhelming number of choices; a curated menu of five to ten measures that cover the key domains relevant to your population is usually enough to support both standardization and personalization.
On the question of program-level versus individualized measures: the panelists recommend a hybrid approach. A small core set of measures, administered consistently across all clients in a program, supports aggregate reporting, quality improvement, and organizational learning. From there, clinicians and clients can add supplementary measures tailored to individual goals, concerns, or presenting issues.
As for “how much is too much”: when MBC is truly embedded into care rather than layered on top of it, it rarely feels excessive. Dr. Barber shared an example of a client who, when offered the option to stop using measures showing stable scores, actually asked to keep them, because the consistency was reassuring and the measures had become a meaningful part of their care experience. The key is integrating MBC into workflows from the start, rather than treating it as a separate administrative task.
How do we reduce administrative burden and ensure MBC feels clinically relevant rather than just additional documentation?
Co-design is the answer Dr. Scott returned to repeatedly in her implementation work at the Healing Measurement Center. Rather than rolling out a standardized MBC system from the top down, the most effective implementations involve clinical leaders, frontline counselors, and clients in designing workflows together.
Specific strategies include: fitting MBC into existing clinical touchpoints rather than creating parallel processes; using technology or EHR integration to surface measure results in real time without requiring manual data entry; and reviewing what existing documentation is actually required versus what has accumulated over time through inertia. Dr. Scott described doing formal de-implementation reviews with sites to identify and remove outdated or redundant paperwork, which creates the space and time for MBC to fit without expanding overall burden.
Is there an efficient way to prevent staff from treating MBC as a checklist rather than a clinical tool? What CQI approaches help?
This challenge (i.e. measures being completed without being meaningfully discussed) is one of the most common barriers to realizing MBC’s clinical value. A few strategies that tend to help:
(1) First, training needs to go beyond the mechanics of completing measures and address the “how” of using data in session. The Collect, Share, Act model is specifically designed to support this. It provides a practical framework for reviewing scores collaboratively with clients, exploring what the data means, and deciding together what to do next. The Yale MBCC Hub includes videos and resources on exactly this, including how to introduce MBC to clients and facilitate these conversations effectively.
(2) Second, embedding MBC review into supervision and team meetings reinforces that data is for clinical use, not just compliance. When supervisors regularly ask how measures are informing treatment decisions, clinicians internalize the difference between checkbox completion and genuine clinical practice.
(3) Third, telling stories matters. Dr. Barber emphasized throughout the webinar that hearing peers share “magic moments” when a measure opened an unexpected conversation or revealed something clinically important, is one of the most powerful ways to shift the culture around MBC. Organizations that create space for these stories, whether in supervision, team huddles, or written case examples, tend to see more sustained and meaningful adoption.
What is the most accessible way to train a large, diverse integrated workforce (nurses, social workers, counselors) to use MBC data more effectively?
Training a broad, multi-disciplinary workforce is one of the most common implementation challenges, and it’s worth addressing in layers.
At the foundational level, all staff who interact with clients and measures need to understand why MBC matters and what it looks like in practice, not just how to administer a screener. Short, role-specific training that grounds MBC in clinical examples from SUD care tends to land better than generic instruction.
At the skill-building level, the Collect, Share, Act model provides a concrete and teachable structure for using measures in session. The Yale MBCC has produced practical training resources that can be used in team training or embedded in onboarding. These are accessible through the Yale MBCC Hub.
At the ongoing support level, identifying clinical champions who have adopted MBC well and empowering them to mentor colleagues is consistently one of the most effective levers. Champions can answer practical questions, share real examples, and make the value of MBC concrete in ways that formal training often can’t.
Working with Specific Populations
How can MBC be helpful in lower-income communities where clients may not have regular access to cell phones or electronics?
Technology access is a real implementation consideration, and the answer is flexibility in how measures are administered. MBC can be delivered through multiple channels — paper forms, clinic kiosks or tablets, staff-assisted completion during session, or remote delivery via SMS or email for clients who do have device access. The clinical process and value of MBC does not require a smartphone.
For populations with limited technology access, building assessment completion into the care encounter as a natural part of intake, check-in, or session start, is often the most reliable approach. When clients complete measures with staff present, it also creates an immediate opportunity to discuss responses and begin the “share” step of Collect, Share, Act, rather than waiting for scores to arrive asynchronously.
Greenspace supports all of these delivery methods, allowing organizations to configure assessment workflows that match their clinical setting and client population.
For adolescents, we work with families and caregivers as part of treatment. If we add caregiver measures, does this make things too complicated?
It doesn’t have to, but it does require thoughtful planning. A few considerations:
- Start simple. Before adding caregiver measures to every case, consider piloting with a subset of families and learning what works in your setting. A brief, validated caregiver report measure that covers the same or complementary domains as the youth’s self-report can add meaningful information without dramatically increasing burden.
- Be explicit about how data will be used and shared. Adolescents and caregivers both need to understand what will be done with their responses, and there are important confidentiality considerations, particularly around substance use disclosure, that need to be addressed in your protocols before introducing caregiver measures.
- Use discrepancies clinically. When youth and caregiver reports diverge, that’s not a problem; it’s clinically useful information. A structured conversation about different perspectives can strengthen the therapeutic relationship and help align everyone on treatment goals. The Collect, Share, Act model applies equally well to multi-informant data.
Client Resistance and Engagement
Some clients resist MBC, similar to how they resist treatment plans. How do you respond to those clients?
Resistance to MBC is often resistance to feeling evaluated or surveilled, which is a particularly understandable response in SUD care, where clients may have histories of stigma, shame, or coercive treatment experiences. A few approaches that help:
- Reframe the purpose explicitly. MBC is not about judgment or compliance, it’s a tool for the client to communicate how they are doing, to see their own progress, and to guide what happens in treatment. When clients understand that measures exist to serve them, not to report on them to funders or administrators, resistance often softens.
- Involve clients in choosing measures. When clients have some say in which domains are tracked, what matters to them, and what they want to pay attention to, they tend to experience MBC as more relevant and less imposed.
- Start with quality of life or recovery-oriented measures rather than symptom or use-focused ones. For clients who are already sensitive about their substance use, beginning with measures that surface strengths, values, and wellbeing can be a lower-stakes entry point that builds engagement before introducing more clinical metrics.
- Use measures in session, visibly and collaboratively. Clients who see their scores reviewed and discussed in real time and who experience MBC as a genuine conversation rather than data collection, are much more likely to find it meaningful. Dr. Barber described a client who, after consistently seeing a happiness item on their measure, began noticing small moments of joy in their daily life between sessions, a spontaneous and therapeutic effect of the measurement process itself.
Is there value in more frequent, shorter interactions that use targeted questions to help clients track their progress and see how treatment is improving their life?
Yes, and this reflects exactly the intent of MBC as a clinical practice. The goal is not simply to accumulate data points, but to create regular, structured opportunities for clients to pause, reflect, and recognize their own progress or identify what’s not working. Research consistently shows that this kind of feedback-informed care improves outcomes and reduces dropout.
Frequent, brief check-ins can be particularly valuable in SUD care, where week-to-week fluctuation is common and small positive changes (i.e. improved sleep, stronger social connection, reduced cravings) may not register as meaningful to a client unless they are made visible. Tracking these shifts over time and showing clients their trajectory can build the sense of agency and momentum that supports continued engagement and recovery.
The key is that data collected must be discussed. Completing measures without reviewing them together removes the clinical value entirely.
Data, Outcomes, and Making the Business Case
As a clinical leader trying to build a business case for MBC in a SUD organization, what quality and ROI arguments are most compelling?
Dr. Scott addressed this directly, and her answer mirrors what Greenspace hears consistently from partners across the sector.
The strongest quality arguments center on: (1) improved treatment alliance and engagement; (2) earlier identification of non-response, allowing timely treatment adjustments; (3) better retention in care, which is a chronic challenge in SUD services; and (4) more consistent clinical formulation and documentation across large, complex caseloads.
From an ROI perspective, organizations that implement MBC with fidelity, meaning they actually discuss and act on data, not just collect it, see measurable improvements in client outcomes that support contract renewals, value-based care arrangements, grant reporting, and accreditation requirements.
Dr. Resnick added a point about sequencing: before aggregated data becomes meaningful for program-level reporting, you need high enough adoption at the clinician and client level. The business case for MBC starts with the clinical case, where organizations use success stories, improved outcomes, and clinician testimonials to build internal momentum. Aggregate reporting value follows as uptake increases.
For organizations still building that internal case, Greenspace’s ROI Calculator can help quantify the potential impact of MBC implementation on outcomes and costs.
How do you summarize the impact of a program when using multiple measures? Which do you select for pre-post evaluation when you have many measurements?
This is both a methodological and a communication question, and the answer depends on your audience.
For internal quality improvement, trend data on a core set of measures, ideally the same small set administered consistently across your client population, gives you the most actionable picture. Measures with reliable change benchmarks (such as the PHQ-9 or GAD-7, which have published minimal clinically important difference thresholds) allow you to report on the percentage of clients who achieved reliable improvement, not just average score changes.
For external reporting to funders, payers, or accreditation bodies, select measures that align with the outcomes those stakeholders care about and that are recognized in the field. For SUD, this often includes substance use frequency or severity, quality of life, and functional status. HEDIS measures (see the question below) may also shape what you report to behavioral health managed care organizations.
When communicating impact broadly, pair quantitative outcome data with qualitative case examples. Numbers alone rarely move people; a concrete story of how a client’s trajectory changed because of an MBC-informed treatment adjustment makes the value of the data legible to non-clinical audiences.
How does MBC tie into HEDIS and the SUD measurements HEDIS is looking to enforce?
HEDIS (Healthcare Effectiveness Data and Information Set) includes several SUD-related measures that behavioral health and integrated care organizations increasingly need to report on, including measures related to initiation and engagement in SUD treatment (IET), follow-up after emergency department visits for alcohol and drug use (FUA/FUD), and more recently, outcome-focused measures for alcohol and drug use disorders.
MBC directly supports performance on these measures by creating consistent, documented evidence of clinical engagement, treatment monitoring, and response to deterioration. Organizations that implement MBC well are typically in a stronger position on HEDIS SUD metrics because they have systematized the clinical processes those metrics are designed to incentivize.
That said, MBC should not be designed around HEDIS. The clinical value comes first, and the compliance benefits follow from genuine implementation. If you’re designing your MBC program primarily to check HEDIS boxes, you’re likely to end up with a measure-collection process that doesn’t improve care, which ultimately won’t serve either goal.
Measuring Harm, Risk, and Level of Care
ASAM Level of Care criteria focuses on the likelihood of harm occurring as a key indicator. What standardized measurement exists for the concept of “harm”?
The panelists were direct about this: there is no widely used, validated measure in the MBC literature that is specifically designed to assess “harm” as ASAM defines it for level of care determination. That is an important gap.
What MBC can do in this context is support the broader clinical judgment process around level of care. By tracking symptom severity, functional status, and risk indicators over time, MBC data provides a structured evidence base for decisions about whether a client needs a higher or lower level of care. It ultimately helps flag when someone isn’t responding to the current level of treatment, when withdrawal symptoms or cravings are worsening, or when social and environmental risk factors are intensifying.
Dr. Resnick also noted an important distinction: not all clinical assessment is MBC. Standardized assessments used for level of care determination, harm assessment, or diagnostic purposes are distinct from the routine outcome monitoring that defines MBC. The ASAM criteria process involves clinician-administered structured assessment tools that are different in purpose and design from the patient-reported outcome measures used in ongoing MBC practice. Both have a role and serve complementary functions in a well-structured SUD program.
For harm-reduction-oriented organizations specifically, some are using measures of overdose risk (e.g., questions about recent overdose or near-miss, current fentanyl exposure, naloxone access) as supplementary items within their MBC approach, even if these aren’t packaged as formal validated scales. Working collaboratively with clients on these questions within a Collect, Share, Act framework can itself be a form of harm reduction, creating structured opportunities for honest conversation about risk.
Can MBC help identify when a client needs a different level of care?
Yes, and this is one of its most practical clinical uses in SUD settings. As Dr. Scott described, when you are tracking client status over time through MBC, deteriorating scores or persistent non-response to treatment become visible in a way that is harder to see without structured measurement. That data can support a clinical judgment to step up care intensity, refer to a higher level of service, or revisit the treatment plan.
This is particularly important in outpatient SUD settings, where clients may underreport difficulty or deterioration in conversation but communicate it more honestly when completing a self-report measure. MBC creates an additional communication channel — one that is structured and consistent enough to support meaningful level-of-care monitoring over time.
Still have questions?
If you’re interested in learning more about implementing MBC in your SUD program, we’d love to connect. Book a call with a Greenspace implementation specialist, or explore our resources below:
- Yale MBCC Hub — practical guides, videos, and implementation resources from the Yale Measurement-Based Care Collaborative
- Assessments Hub — detailed guidance on over 40 commonly used measures, including SUD-relevant tools
- What is Measurement-Based Care? — an overview of the MBC model and the evidence behind it