Generalized Anxiety Disorder 7 (GAD-7)
Recommended frequency: Every 2 weeks
Summary
The Generalized Anxiety Disorder 7 (GAD-7) instrument is used to measure and monitor the severity of generalized anxiety disorders. The scale was published in 2006 by Robert L. Spitzer, Kurt Kroenke, Janet B. W. Williams, and colleagues, and was designed to be a brief and easy to complete 7-item scale for measuring generalized anxiety, based on criteria outlined in the Diagnostic and Statistical Manual of Mental Disorders-IV (DSM-IV). Evidence has shown that the GAD-7 has effective sensitivity and specificity for screening for other anxiety disorders, such as Panic, Social Anxiety and Posttraumatic Stress Disorders. The measure was originally developed to be used with adults (18+), however it has also been validated for use with adolescents (14-17) with generalized anxiety, as GAD-7 scores can support the assessment of anxiety symptoms and help differentiate between mild and moderate anxiety in youth (Mossman et al., 2018).
About the GAD-7
Despite only recently being developed in 2006, the GAD-7 is one of the most commonly utilized measures for anxiety. There are many other validated measures that exist to identify and monitor anxiety, including the Hamilton Anxiety Scale (HAM-A), Hospital Anxiety and Depression Scale (HADS), Covi Anxiety Scale, Clinical Anxiety Scale (CAS), State-Trait Anxiety Inventory (STAI), Generalized Anxiety Disorder Questionnaire-IV (GAD-Q-IV), and World Health Organization Composite International Diagnostic Interview Short-Form (CIDI-SF), among others.
The GAD-7 was developed based on the 9 symptom criteria for generalized anxiety in the DSM-IV in addition to to 9 questions.
To create the measure, the authors identified an initial list of potential items that could compose the scale. They started with 9 items that each corresponded to symptom criteria for generalized anxiety disorders within the DSM-IV, plus 4 additional items based on a fulsome review of other existing anxiety scales. Their goal was to identify the items that were most effective at measuring anxiety symptoms and shorten the length of the measure, in order to reduce assessment burden on patients and increase completion rates, while ensuring strong reliability and procedural, construct, and diagnostic criterion validity.
In order to do so, they completed a criterion-standard study that compared GAD self-report scale diagnoses to independent diagnoses made by mental health professionals, as well as functional status measures, disability days, and health care use. There were two phases to this project, the first being to identify the scale items and determine cut off scores, and the second focused on testing its reliability. The final 7 items were chosen based on them having the highest correlation with the total 13-item scale score (Spitzer et al., 2006).
When scoring the GAD-7, the authors recommend using a cut off score of 10 which ensures a sensitivity of 89% and a specificity of 82% for generalized anxiety disorders— meaning a score of 10 or higher on the GAD-7 is a good indication of potential Generalized Anxiety Disorder diagnosis (Spitzer et al., 2006). The measure can also assist with detecting three other common anxiety disorders, including Panic Disorder (sensitivity 74%, specificity 81%), Social Anxiety Disorder (sensitivity 72%, specificity 80%), and Post-Traumatic Stress Disorder (sensitivity 66%, specificity 81%) (Spitzer et al., 2006).
Assessments on Greenspace
Interested in learning more about how Greenspace can simplify and enhance your measurement practice?
Book a CallWho is the GAD-7 Assessment for?
Review the list below to determine if this assessment should be used with your client. If you answer NO the below question, the GAD-7 is a good fit to use with your client.
- Is your client under 14? If they are, please refer to the Child Depression & Anxiety (RCADS 25) measure.
Note: The GAD-7 has shown good sensitivity, specificity, reliability, and factorial, construct, and concurrent validity in many specific subgroups, including patients with chronic migraines (Seo and Park, 2015), drug and alcohol use challenges (Delgadillo et al., 2012), as well as elderly people (Wild et al., 2014), and pregnant women (Zhong et al., 2015). Seeing that it is short and easy to administer, it is also effective in multiple settings, such as remote health surveys, epidemiologic studies, primary care, and in-person settings (García-Campayo et al., 2012).
Administering the GAD-7
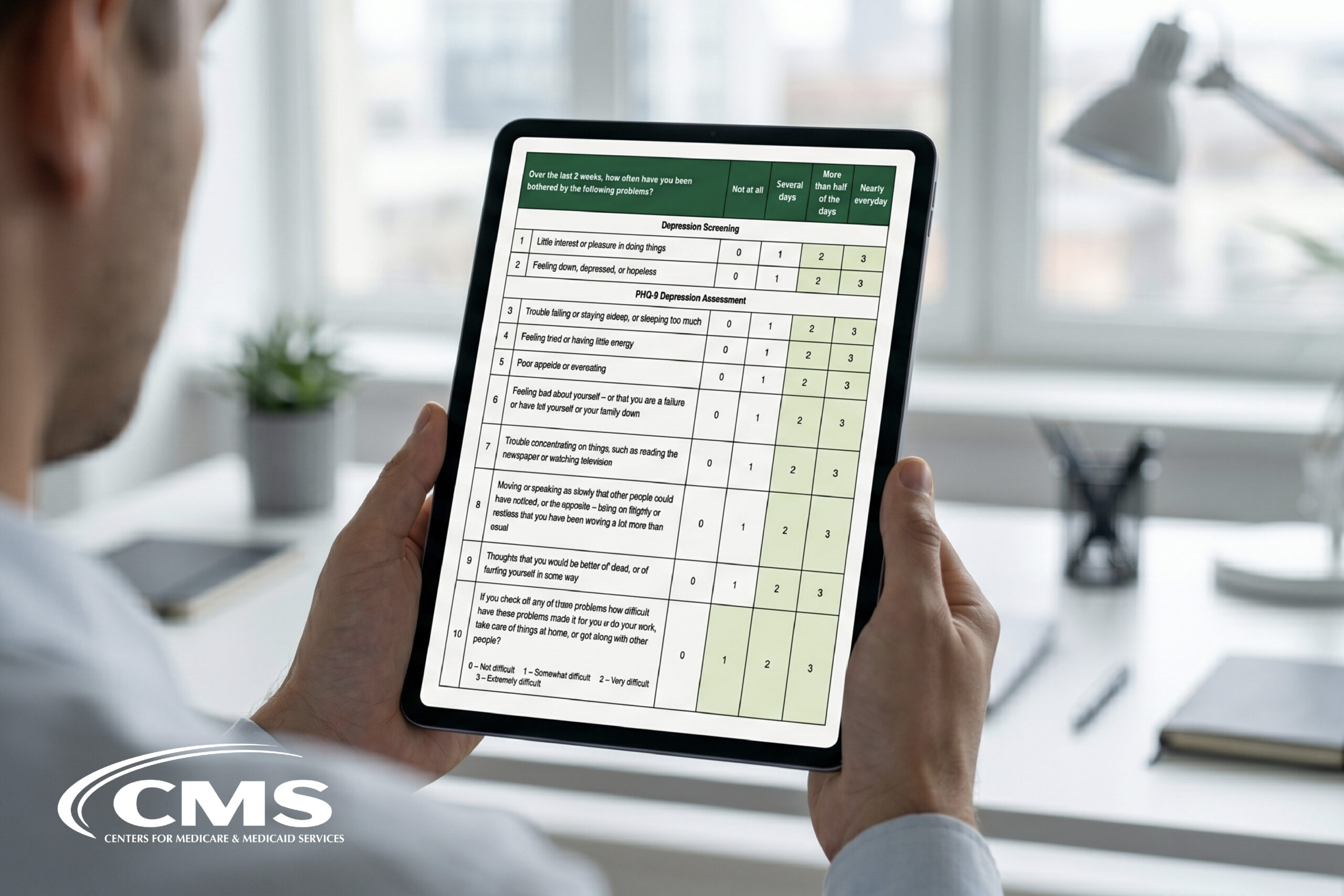
The GAD-7 asks respondents how often, during the last 2 weeks, they were bothered by each of the 7 items. Response options are “not at all,” “several days,” “more than half the days,” and “nearly every day,” each scored as 0, 1, 2, and 3.
Though this is a self-report measure, validity is not compromised if the therapist reads the questions to the client to help them complete it. The scale can be administered by non-clinical staff, but must be interpreted by a licensed clinician. If administering the scale over the phone, it is important to ensure the client can recall and implement the response scale when scoring each item. While the scale (shown below) has intentionally developed to be easy to understand for clients, it may be beneficial to review the scale questions when first introduced and to revisit or check in on a clients’ interpretation of questions at regular intervals throughout their time in care.
Watch this video from Buckinghamshire Healthcare NHS Trust, filmed at Mandeville Hospital, to see an example of the assessment being administered verbally in session. Notice how the client is actively interpreting the questions and discussing how his answers may apply, while the provider is asking clarifying questions when necessary to ensure the most accurate responses. This is an important process to ensure the client has an appropriate interpretation of the question and can recall moving forward.
Video Credit: buckshospitals
The GAD-7 Scale
Over the last 2 weeks, how often have you been bothered by the following problems?
| Not at all | Several days | More than half the days | Nearly everyday | |
|---|---|---|---|---|
| 1. Feeling nervous, anxious, or on edge | 0 | 1 | 2 | 3 |
| 2. Not being able to stop or control worrying | 0 | 1 | 2 | 3 |
| 3. Worrying too much about different things | 0 | 1 | 2 | 3 |
| 4. Trouble relaxing | 0 | 1 | 2 | 3 |
| 5. Being so restless that it is hard to sit still | 0 | 1 | 2 | 3 |
| 6. Becoming easily annoyed or irritable | 0 | 1 | 2 | 3 |
| 7. Feeling afraid as if something awful might happen | 0 | 1 | 2 | 3 |
Scoring the GAD-7
Anxiety severity is calculated by assigning scores of 0, 1, 2, and 3, to the response categories of “not at all”, “several days”, “more than half the days”, and “nearly every day”, respectively. The total GAD-7 score for the seven items can range from 0 to 21.
The following cut-offs can be used to determine severity of anxiety:
| Score | Anxiety Severity |
| 0-4 | None – Minimal |
| 5-9 | Mild |
| 10-14 | Moderate |
| 15-21 | Severe |
Though the authors recommend a cut-point of 10 for anxiety disorder screening, a recent meta-analysis suggests utilizing a cut-off of 8 in order to optimize sensitivity without compromising specificity (Plummer et al., 2016). A score of 8 or greater represents a reasonable cut-point for identifying probable cases of Generalized Anxiety Disorder; however, further diagnostic assessment is warranted to determine the presence and type of anxiety disorder. When using a cut-off of 8, the GAD-7 has a sensitivity of 92% and specificity of 76% for the diagnosis of Generalized Anxiety Disorder (Plummer et al., 2016).
Screening for other anxiety disorders with the GAD-7
As mentioned previously, though the GAD-7 was designed primarily as a screening and severity measure for Generalized Anxiety Disorder, it also has moderately good operating characteristics for three other common anxiety disorders, including Panic Disorder, Social Anxiety Disorder, and Post-Traumatic Stress Disorder (Kroenke et al., 2007).
| Performance of GAD-7 as Screening Tool for Anxiety Disorders (Using GAD-7 Score Cut-off of ≥ 10) |
|||
|---|---|---|---|
| Test | Sensitivity | Specificity | Positive Likelihood Ratio |
| Generalized Anxiety Disorder | 89% | 82% | 5.1 |
| Panic Disorder | 74% | 81% | 3.9 |
| Social Anxiety Disorder | 72% | 80% | 3.6 |
| Post-Traumatic Stress Disorder | 66% | 81% | 3.5 |
| Any anxiety disorder | 68% | 88% | 5.5 |
If other mental health challenges are present, evidence shows that adding a more precise measure in response to clients’ unique challenges drives improved clinical outcomes throughout treatment. For example, if a client is struggling with anxiety but you suspect it might be linked to PTSD, it can be beneficial to add a PTSD specific measure as it will be more sensitive to the unique symptoms present in this condition. Watch the clip below where Dr. David Clark (Clinical and Informatics Advisor, NHS, and Chair of Experimental Psychology, Oxford University) shares the results of this impact across the NHS Talking Therapies program, where the responsive addition of an additional measure specific to a client’s challenges increases the number of sessions completed within a clients’ treatment plan and improves the effectiveness of care, resulting in higher recovery rates among these individuals:
Diagnosis
If considering a diagnosis for anxiety, you should hold a clinical interview to determine if symptoms and distress levels outlined in GAD-7 results are clinically significant. It is also important to rule out other explanations or existing conditions that may lead to the presenting anxiety symptoms, including substance use, medical conditions, bereavement, or anything other factors that may be impacting your client.
Applying GAD-7 Results in Session
Now that you’ve started using the GAD-7 in session with your client(s), it’s important to leverage the information you’re gathering to inform clinical discussions, treatment decisions and improve both therapeutic alliance and clinical outcomes. Here are a few ways you can incorporate the GAD-7 results throughout care:
Treatment Planning
The information gathered by this measure can support and enrich clinical conversations, in order to give you a more complete picture of your clients experience. In addition to leveraging results to inform care discussions, decisions and treatment planning, GAD-7 scores can also be leveraged to inform additional techniques, interventions, exercises and referrals to improve care, based on each item of the GAD-7 (developed by VISN 4 MIRECC). Explore the additional suggestions below that can be considered for clients experiencing challenges with any of the 7 items:
1. Feeling nervous, anxious or on edge:
- Diaphragmatic breathing
- Thought monitoring
- Challenging maladaptive thoughts/feelings
2. Not being able to stop or control worrying.
- Identifying maladaptive thoughts/ feelings
- Challenging maladaptive thoughts/feelings
- Relaxation techniques
3. Worrying too much about different things.
- Thought monitoring
- Solvable vs. Unsolvable worries
- Identify possible solutions
4. Trouble relaxing
- Diaphragmatic breathing
- Autogenic Relaxation
- Guided Imagery
5. Being so restless that it is hard to sit still
- Diaphragmatic breathing
- Progressive Muscle Relaxation
- Guided imagery
6. Becoming easily annoyed or irritable
- Challenging maladaptive thoughts/feelings
- Breathing techniques
- Identify consequences to actions
7. Feeling afraid as if something awful might happen
- Thought monitoring
- Solvable vs. Unsolvable worries
- Challenging maladaptive thoughts/feelings
If you have any more questions about how to leverage assessments in session or how to use scores to guide clinical discussions or decision making, visit our Assessment Hub for more information.
Monitoring Progress and Change
Leveraging the GAD-7 throughout care helps both you and your client monitor progress in treatment and serves as an indicator of when things may not be improving. If a client scores less than 5 on 2 or more assessments in a row (with a minimum of 2 weeks between each assessment), there is good reason to believe that your client may be ready to discharge or transition into maintenance treatment.
Delgadillo, J., Payne, S., Gilbody, S., Godfrey, C., Gore, S., Jessop, D., & Dale, V. (2012). Brief case finding tools for anxiety disorders: validation of GAD-7 and GAD-2 in addictions treatment. Drug and alcohol dependence, 125(1-2), 37–42. https://doi.org/10.1016/j.drugalcdep.2012.03.011
García-Campayo, J., Zamorano, E., Ruiz, M. A., Pérez-Páramo, M., López-Gómez, V., & Rejas, J. (2012). The assessment of generalized anxiety disorder: psychometric validation of the Spanish version of the self-administered GAD-2 scale in daily medical practice. Health and quality of life outcomes, 10(114). https://doi.org/10.1186/1477-7525-10-114
Kroenke, K., Spitzer, R. L., Williams, J. B., Monahan, P. O., & Löwe, B. (2007). Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Annals of internal medicine, 146(5), 317–325. https://doi.org/10.7326/0003-4819-146-5-200703060-00004
Sapra, A., Bhandari, P., Sharma, S., Chanpura, T., & Lopp, L. (2020). Using Generalized Anxiety Disorder-2 (GAD-2) and GAD-7 in a Primary Care Setting. Cureus, 12(5), e8224. https://doi.org/10.7759/cureus.8224
Seo, J. G., & Park, S. P. (2015). Validation of the Generalized Anxiety Disorder-7 (GAD-7) and GAD-2 in patients with migraine. The journal of headache and pain, *16(*97). https://doi.org/10.1186/s10194-015-0583-8
Spitzer, R.L., Kroenke, K., Williams, J.B.W., Löwe, B. (2006). A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. *Arch Intern Med, 166(*10). 1092–1097. https://doi.org/10.1001/archinte.166.10.1092
Zhong, Q. Y., Gelaye, B., Zaslavsky, A. M., Fann, J. R., Rondon, M. B., Sánchez, S. E., & Williams, M. A. (2015). Diagnostic Validity of the Generalized Anxiety Disorder – 7 (GAD-7) among Pregnant Women. PloS one, 10(4), e0125096. https://doi.org/10.1371/journal.pone.0125096
Other resources
VISN 4 MIRECC. (n.d.) GAD_with_Info_Sheet.pdf. Veterans Affairs. https://www.mirecc.va.gov/cih-visn2/Documents/Clinical/GAD_with_Info_Sheet.pdf
Copyright
Developed by Drs. Robert L. Spitzer, Janet B.W. Williams, Kurt Kroenke and colleagues, with an educational grant from Pfizer Inc. No permission required to reproduce, translate, display or distribute.
Explore More Assessment Insights
Check out more than 40 Assessment Guides with information and insights on the most popular assessments used on the Greenspace MBC Platform. Explore the categories below to find assessments you may be interested in learning more about.
Back to the hub